Suporn Method Vaginoplasty
A lot of people have written in depth about their experiences of vaginoplasty and the process involved in getting it. I am not gonna do better than this obsessively in-depth experience report. So I thought I'd rather write something about the scientific and surgical aspects of Suporn Method vaginoplasty, as there seems to be a lot of confusion and misconceptions about this method and vaginoplasty in general.
Some Useful Terms
In order to illustrate what this surgery is and distinguish it from other methods let me define a few terms: a pedicle flap is when tissue is moved around without being fully detached from its original site, so that it can continue to draw from its original blood supply. A free flap is probably what you think of when you think about tissue grafting – tissue is taken from one place and moved, with its blood supply, to another place, where the blood supply is reconnected. A graft is like a free flap but the blood supply isn't taken along with the tissue – this involves less microsurgery but the transplanted tissue needs to have an adequate blood supply from the surrounding area while it regrows its own blood vessels.
Penile Inversion
This is the oldest and most commonly-performed style of vaginoplasty. The corpora cavernosa (the erectile tissue of the penis) are removed and the penile skin is degloved and inverted to become the vaginal canal. This is done as a pedicle flap. The testicular skin then is typically used to form the labia and the glans, or part of it, is used to form the clitoris (also pedicled).
The key limitation of this technique is that the depth and width of the vagina are limited by the amount of penile skin. Given that long-term estrogen exposure can lead to penile atrophy and loss of volume, and that trans women who transition early may not even experience full development of penile volume, this is a serious limitation.
Another limitation is that scrotal skin is not really the appropriate homologous tissue for the labia minora and vulval vestibule. It is not pink and it can be more or less sensitive. The color can be adjusted later with medical tattooing but requires a second procedure with a different specialist later.
The big advantage of this method is that with some clever cuts you can preserve the whole original topology and maintain the original blood supply everywhere, which greatly eases recovery.
Suporn Method
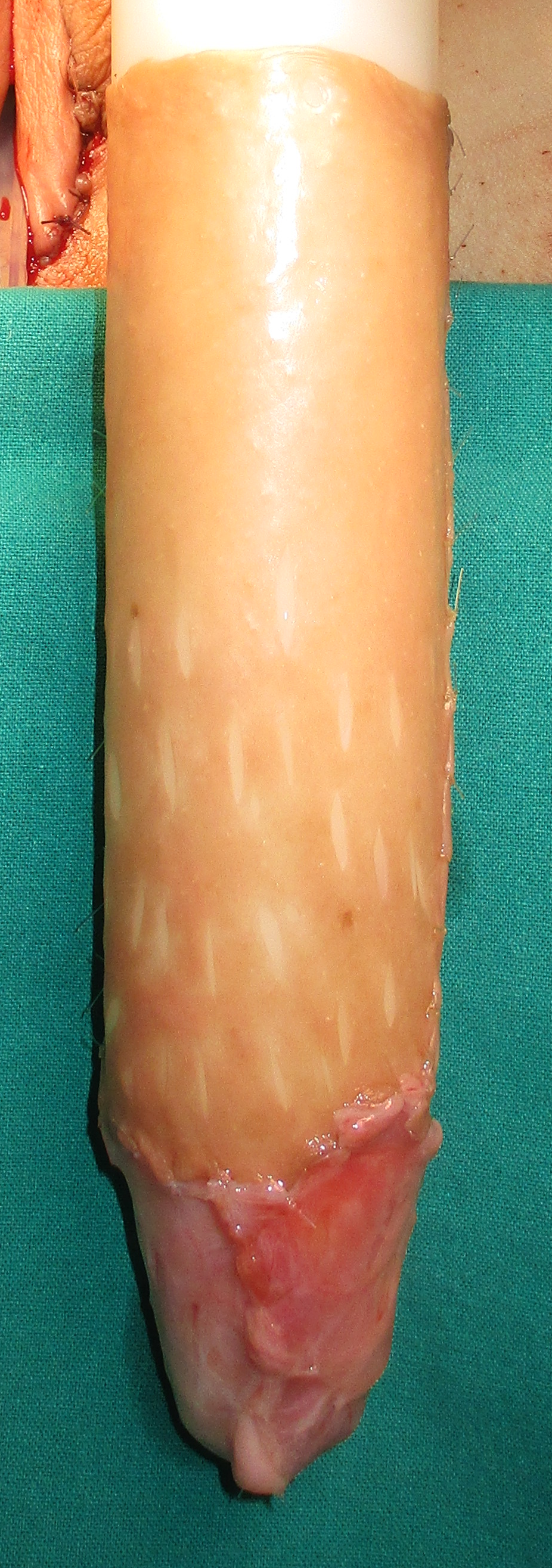
This is one of a broad class of non-penile inversion vaginoplasty methods. In this method, which would be called a "scrotal skin graft partial-peritoneal vaginoplasty" if plastic surgeons weren't psychotic egotists, a scrotal skin graft is used to create the vaginal canal instead of a penile skin flap. The scrotal skin is processed in an unclear way that results in the removal of hair follicles and a fleshy appearance. Since in a penile inversion vaginoplasty there is typically an excess of scrotal skin that ends up getting thrown away, here is plenty of scrotal skin left over to form the labia majora as well.
Using scrotal skin rather than penile skin for the vaginal canal has a few big advantages:
- It frees the penile skin to be used to form the vestibule of the vagina and the labia minora, for which it is a better tissue homologue.
- It provides an unlimited amount of skin (relative to the amount of free space in the pelvis) so that a patient can expect 14 cm or more of depth.
- The scrotal skin is being processed anyway so extensive hair removal beforehand is not necessary
The disadvantage is that because the vaginal canal is a graft, it has much more healing to do and recovery can be more harsh. It personally took me over a month before I could really do much walking around and I was in the hospital for a week.
There are two additional aspects of the Suporn Method worth mentioning
Tunica Vaginalis
Something the Suporn clinic seems to have started doing in the last few years is using the tunica vaginalis for the deepest few centimeters of the vagina. The tunica vaginalis is a serous membrane surrounding the testes. Including it provides a builtin source of lubrication. It is homologous to peritoneal tissue so the result is very similar to the peritoneal pullthrough method, another non-penile inversion vaginoplasty method.
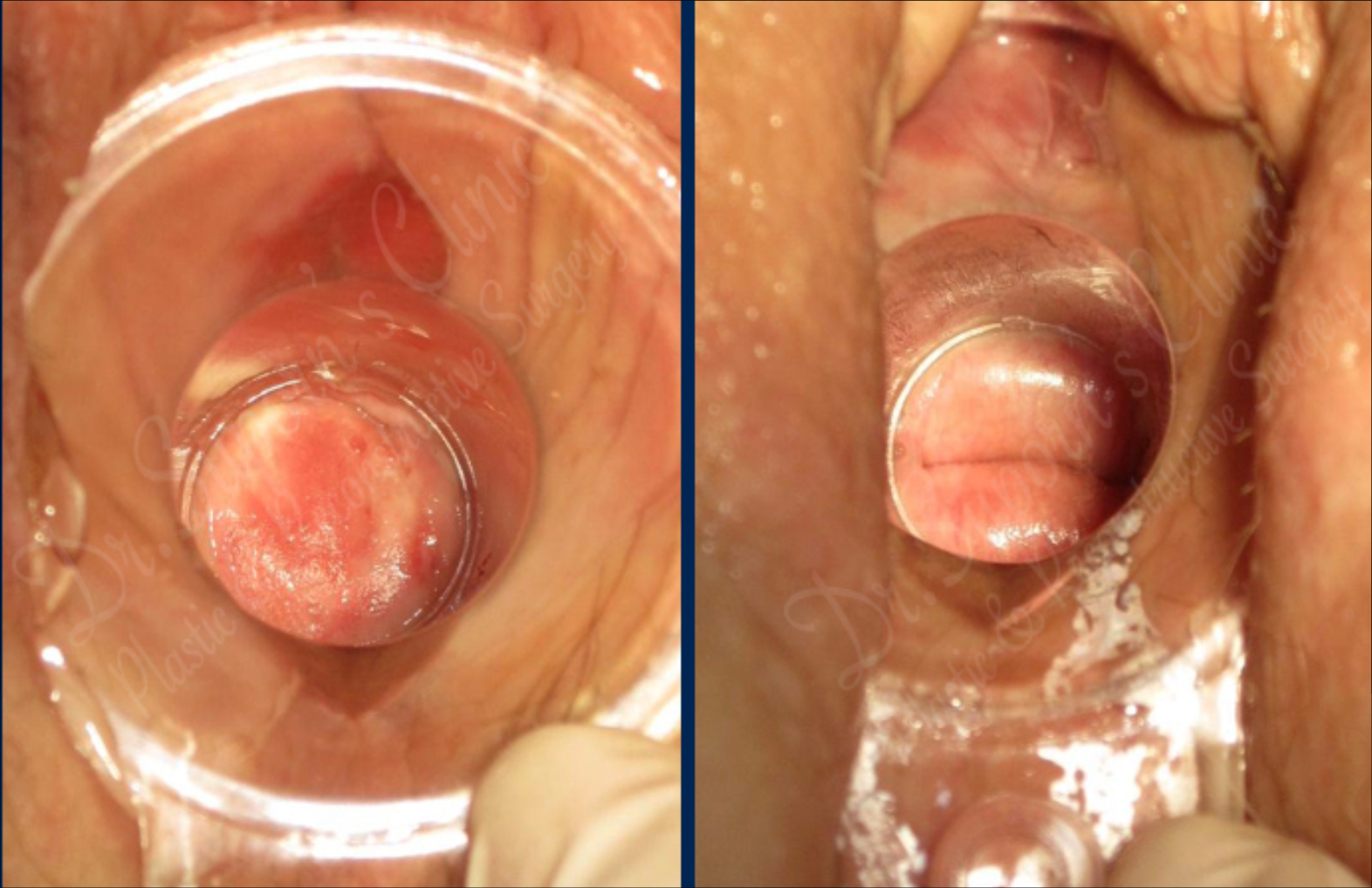
Chonburi Organ
The new glans clitoris seems to be the structure most prone to necrosis as it's healing. Total loss seems very rare but just in case the Suporn clinic creates a second clitoris structure below the first which is informally called the Chonburi organ. Since the glans penis is oversized for a clitoris this is no problem.
Processing of the Scrotal Skin
I have tried to figure out exactly how the scrotal skin that produces the vaginal canal is processed. As far I can tell, there is no official source that lays this out in detail, other than to say it is a "full thickness genital skin-mucosal graft." What I think is happening is that a full-thickness graft is taken, defatted, then placed so that the keratinized hair-bearing side is facing the wound bed and the mucosal previously-interior side is now exterior, composing the vaginal canal. Then the keratinized outer-layer is naturally resorbed and destroyed by the body. Another possibility is that "full thickness" here refers to the thickness at the point it is harvested (since the site is being destroyed anyway), and that before implantation the bottom layer of the dermis is removed. That would make the graft, once transplanted, functionally equivalent to a split-thickness graft.
click to reveal
click to reveal
Major structures and Homologies
Here's an overview of the structures of the vulva and where they come from in the Suporn method:
| Female structure | Male structure | Homology |
|---|---|---|
| Glans clitoris | Glans penis | Direct homology |
| Labia majora | Scrotum | Direct homology (you can see where they join developmentally in the Raphe line) |
| Labia minora | Penile skin | Direct homology (you can see this in the penile Raphe) |
| Vagina | Scrotum/tunica vaginalis | Not homologous (the vagina develops from the Müllerian ducts which are broken down during male fetal development so there is no remaining homologous tissue) |
| Urethra | Urethra | It's just shortened |
Myths and Misconceptions
There are a lot of misconceptions about neovaginas which I see commonly repeated even among trans people. I will try to correct them here.
The neovagina is not self-lubricating or at least not self-lubricating enough for sex
There is no biologically principled reason to believe this is the case. Natal vaginal lubrication is mainly plasma transudate. It is not mainly glandular or mucosal or some special type of tissue. The graft tissue should do this exactly the same if it is thin, non-keratinized, and well-vascularized, which in the case of this method it will be. My neovagina has a normal level of self-lubrication.
The neovagina will close up if dilation is ceased
This is sometimes also stated as "the body will consider it a wound forever and try to close it." That's simply not how wound healing works. There is certainly a period of time during which the tissue is healing in which adhesion can cause the neovagina to close up partially or fully. After this period, the tissue is healed and it will not seal itself any more than a natal vagina will, or any more than your toes will graft together from contact.
Rather, the purpose of dilation changes over time. At first, preventing adhesion is important. After the first month or two, it's to do with training the pelvic muscles to adopt a new position and preventing a reduction in vaginal width as the scar rings where the grafts are joined tend to contract as they slowly heal. After 2 years or so, there is no clear purpose for ongoing dilation. My impression is that after this point patients find regular dilation is not necessary, and if you absolutely never dilate you might just have some fixable vaginismus.
The neovagina needs to be regularly douched forever
While the neovagina is healing it puts out lots of pus and blood and needs to be kept somewhat abiotic so it's a good idea to douche regularly. When healing is done, that is no longer necessary. In natal vaginas, douching is not necessary and in fact is unhealthy. The vagina has a microbial film and self-cleaning secretions and neovaginas develop these things too.
I also hear the sub-misconception that neovaginal microbiomes are necessarily different from natal vaginal microbiomes. There is no reason to think that is the case. The vaginal microbiome is low-pH created by lactobacilli, which feed on glycogen. I have heard that graft tissue does not produce glycogen but that isn't well established either. Studies suggest the graft tissue is likely to undergo metaplastic adaptation, which should allow it to produce glycogen. (And prepubescent girls, postmenopausal women, and transgender men on testosterone all have healthy [though different] vaginal microbiomes without glycogen as the release of glycogen in these tissues is mediated by estrogen levels.) The conditions under which this takes place are completely unresearched.
There is a reduction in sensation associated with vaginoplasty
Of course this is a risk with any plastic surgery but this wasn't the case at all for me. I find my vagina is far more sensitive than my previous genitals ever were. I can only speculate on why this might be but it's not a subtle difference. I can have continuous or serial orgasms that are far more enjoyable than penile orgasms.
Why do these myths arise?
I speculate that these myths arise due to the inherent conservatism of doctors. They don't want to promise anything that they can't guarantee they will deliver. And there is very little followup on vaginoplasty. Doctors essentially never follow up after a year, two years, five years. Therefore, doctors are not willing to make promises about what tissues will do after they have arranged them into place. Transgender women then assume that they are making evidence-based claims, which they are not.
Interesting Papers
Adaptation process of the skin graft to vaginal mucosa after McIndoe vaginoplasty suggests that graft-based neovaginas are histologically and biologically normal. Unfortunately a followup study on full-thickness grafts which would have been very enlightening seems not to have ever been published. The most well-known paper suggesting the opposite is probably Do Histologic Changes in the Skin-Lined Neovagina of Male-to-Female Transsexuals Really Occur? - this study was conducted on keratinized penile and scrotal skin flaps i.e. tissue of a completely different character. Role of progenitor cell producing normal vagina by metaplasia in laparoscopic peritoneal vaginoplasty shows that peritoneal tissue (of which tunica vaginalis is an example) undergoes metaplasia in neovaginas.
There is a similar story on other topics. The quality of research is generally very poor. Vaginal self-lubrication following peritoneal, penile inversion, and colonic gender-affirming vaginoplasty: a physiologic, anatomic, and histologic review is the most commonly cited study on vaginal self-lubrication. Although the conclusion is that "[n]one of penile/scrotal skin, colon, or peritoneum provides functional neovaginal lubrication comparable to that of the adult natal vagina" this is actually just an assertion by the authors based on the assumption of keratinized skin. The data itself is mixed. And the authors were able to find zero studies that actually quantified or analysed secretions. The microbiome of the neovagina: a systematic review and comparison of surgical techniques found that "PIV neovaginas were most similar to cisvaginas [sic...] with bacterial vaginosis." Such as the bacterial vaginosis a "cisvagina" might develop if its bearer's doctor were to tell her to douche every day.
You may also be interested in Suporn's own presentation on this and this great overview.